To reach a scoliosis diagnosis, an X-ray is needed to determine the size of the curve and the presence of rotation. The results of this initial scoliosis X-ray will shape the customization of treatment plans, and measurements taken will be referred to throughout the course of treatment to gauge how the spine is responding.
The potential outcome of a treatment plan can be shaped by a patient’s initial assessment. Was it accurate? How comprehensive was it? Who performed it? When it comes to reading a scoliosis X-ray and measuring scoliosis accurately, this requires the eye of a trained professional.
As a progressive condition, the timing and accuracy of a patient’s diagnosis is key.
Initial Assessment
An initial patient assessment will look for indicators of scoliosis.
From the first visit, the ScoliCare approach is patient-centered and focuses on how to achieve the best potential treatment outcome, and our experienced team of Clinicians understands the importance of a patient’s initial assessment.
An initial assessment will involve taking a patient’s family history, medical history, and a comprehensive physical examination that observes posture, movement, and includes an Adam’s forward bend test (1).
We can tell a lot about the health of a patient’s spine by how they hold their body and move..
Our treatment plans are 100-percent customized and based on the accuracy of information gleaned, and in most cases, the earliest signs of scoliosis involve postural changes such as uneven shoulders, uneven shoulder blades, and one side of the rib cage protruding more than the other (1, 2).
An Adam’s forward bend test is the most common scoliosis screening test and involves examining a patient’s spine and torso while in a forward-bend position; in this position, the spine and any related trunk asymmetries are highly visible and easier to detect (2).
An Adam’s test can be combined with the use of a scoliometer to indicate a patient’s angle of trunk rotation (ATR).
So if a patient’s initial assessment finds indicators of scoliosis, further assessment is warranted in the form of a scoliosis X-ray.
Scoliosis X-ray: What it Tells Us
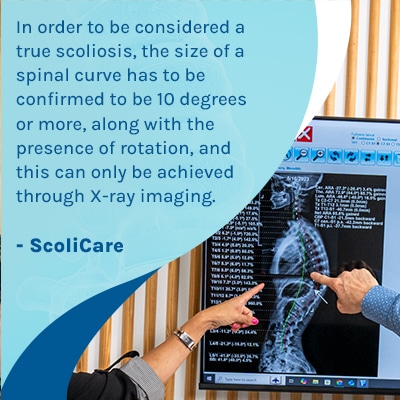
In order to be considered a true scoliosis, the size of an unnatural spinal curve has to be confirmed to be 10 degrees or more, along with the presence of rotation, and this can only be achieved through X-ray imaging.
Our ScoliCare Clinicians understand the importance of the first scoliosis X-ray as it will shape the design of treatment plans.
Standing X-rays are recommended for scoliosis as a curve’s true degree of alignment can be skewed if a patient is lying down, and this is an insight patients and their families should have (2).
Measurements taken during a first X-ray are referred to throughout a patient’s course of treatment to observe how the spine is adjusting to growth and/or treatment, and treatment disciplines are adjusted and apportioned accordingly based on the comparisons of these measurements.
Cobb Angle
The most significant measurement is known as the Cobb angle, and this measurement determines condition severity; the larger the angle, the larger the curve, and the more severe the condition (1, 2).
A patient’s Cobb angle measurement informs treatment recommendations, and it’s a complex measurement, so needs to be determined accurately and by a scoliosis trained health professional (4).
Risk Factors for Progression
X-rays also involve assessing other important factors like bone maturity in children (3).
Scoliosis is progressive, and while we don’t fully understand the cause of most cases, we do know it’s growth that triggers progression, so patient age is a risk factor for potential progression, but patients grow and mature at different rates, so a more detailed means of assessment is needed when it comes to managing a patient’s potential progression (3).
Assessing bone age on an X-ray gives us more information regarding further spinal growth and a patient’s potential rate of curve progression (3).
Other risk factors in adolescents include the size of the curve and the type of curve (4). For example, the larger curves and single thoracic curves are at higher risk of progression (4). Larger curves (beyond 50 degrees) may require a more aggressive approach and sometimes need surgery (5).
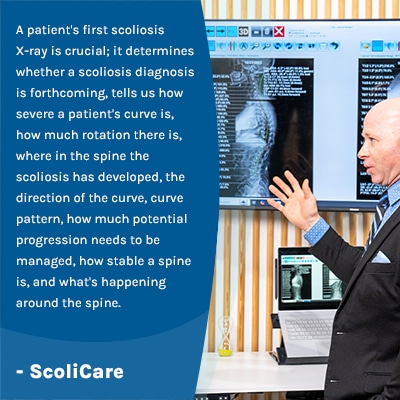
A patient’s first scoliosis X-ray is crucial; it determines whether a scoliosis diagnosis is forthcoming, tells us how severe a patient’s curve is, how much rotation there is, where in the spine the scoliosis has developed, the direction of the curve, curve pattern, how much potential progression needs to be managed, how stable a spine is, and what’s happening around the spine.
So a patient’s initial assessment will determine if enough indicators of scoliosis are present to warrant an X-ray, and a patient’s first scoliosis X-ray will determine whether scoliosis is diagnosed and inform the customization of treatment plans moving forward.
Customizing Scoliosis Treatment Plans
The more specific a patient’s information is, the more customized a treatment plan can be, and the more potential there is for a successful outcome.
So how is the information gleaned during an X-ray actually used?
When it comes to Cobb angle, a measurement of 10+ degrees is the diagnostic cutting-off point, so this is needed to reach a diagnosis of scoliosis (1).
For measurements between 10 and 25 degrees, this is considered mild scoliosis, and patients diagnosed with mild scoliosis are at the beginning of their progressive line, so this means the opportunity to start treatment while curves are mild and easier to correct is within reach (2).
A diagnosis of mild scoliosis in a child means significant progression hasn’t yet been triggered, and this means the scoliosis can be managed through growth, which is associated with treatment success.
So a diagnosis of mild scoliosis doesn’t mean a patient’s scoliosis is minor in any way. It doesn’t indicate a lack of urgency or that there is more time for treatment to unfold; it means early detection has been achieved and early intervention is the next goal (2). All big curves start small, and early intervention minimises the need for surgery (2, 6).
While each case is specific and treatment results can never be guaranteed, in children with mild scoliosis, a customized scoliosis-specific exercise program and part-time corrective bracing are commonly recommended. This approach can help to reduce or stabilise the curve (8) and improve trunk muscle endurance (9) which is important for preventing issues later on (7).
In curves that are larger and measure over 35 degrees, we know more than scoliosis-specific exercises will be needed, and full-time bracing is a primary treatment recommendation (2).
With progressive conditions like scoliosis, the timing of when treatment is started can be an important factor, so the sooner scoliosis is diagnosed, the better as it widens the scope of non-surgical treatment (6).
For curves that are severe and measure over 60 degrees, surgical intervention may be deemed necessary (2). More recently, however, some patients with very large curves have experienced curve improvement or stabilisation with more intensive treatment, but more research is needed (6).
So as you can see, a patient’s Cobb angle alone is a key measurement, and when combined with the other pieces of key information gleaned from an X-ray, it’s clear how a patient’s entire course of treatment is shaped around the accuracy and comprehensiveness of their initial assessment and X-ray images.
Conclusion
What patients and their families need to know about scoliosis is that it can be highly treatable, but some parameters have to be in place to increase potential treatment efficacy: the most important of which is the accuracy of a patient’s initial assessment and X-ray readings.
Scoliosis is a complex progressive condition that’s beyond the scope of general medical treatment; it requires a customized approach crafted by a specialist.
Particularly when it comes to childhood scoliosis, how to manage progression during growth is a challenge, and determining severity, remaining growth, and a number of other variables, helps us come up with a detailed plan.
When it comes to managing scoliosis in older adults, fall prevention is a focus and can only be worked towards if the spine’s balance and stability are accurately assessed and monitored via X-ray.
There are no treatment guarantees, but treatment success is linked with early detection and intervention, so the sooner a diagnosis of scoliosis is reached, the sooner treatment can be started, and this can mean correcting a minor curve before it becomes moderate or severe.
References:
- Weinstein, S. L. (2019). The natural history of adolescent idiopathic scoliosis. Journal of Pediatric Orthopaedics, 39, S44-S46.
- Negrini, S., Donzelli, S., Aulisa, A. G., Czaprowski, D., Schreiber, S., de Mauroy, J. C., … & Zaina, F. (2018). 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis and spinal disorders, 13(1), 3.
- Troy, M. J., Miller, P. E., Price, N., Talwalkar, V., Zaina, F., Donzelli, S., … & Hresko, M. T. (2019). The “Risser+” grade: a new grading system to classify skeletal maturity in idiopathic scoliosis. European Spine Journal, 28(3), 559-566.
- Lenz, M., Oikonomidis, S., Harland, A. et al. Scoliosis and Prognosis—a systematic review regarding patient-specific and radiological predictive factors for curve progression. Eur Spine J 30, 1813–1822 (2021). https://doi.org/10.1007/s00586-021-06817-0
- Bettany‐Saltikov, J., Weiss, H. R., Chockalingam, N., Taranu, R., Srinivas, S., Hogg, J., … & Arnell, T. (2015). Surgical versus non‐surgical interventions in people with adolescent idiopathic scoliosis. Cochrane Database of Systematic Reviews, (4).
- Nalda, A., Mirenzi, R., Doueihi, N. L., & McAviney, J. (2025, June). A Non-Surgical Multimodal Approach to Severe Thoracic Adolescent Idiopathic Scoliosis Combining ScoliBrace and Scoliosis-Specific Rehabilitation Therapies: A Case Series. In Healthcare (Vol. 13, No. 13, p. 1522). MDPI.
- Negrini, S., Grivas, T. B., Kotwicki, T., Maruyama, T., Rigo, M., Weiss, H. R., & members of the Scientific society On Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) stefano. negrini@ isico. it. (2006). Why do we treat adolescent idiopathic scoliosis? What we want to obtain and to avoid for our patients. SOSORT 2005 Consensus paper. Scoliosis, 1(1), 4.
- Bettany Saltikov, J., Parent, E., Romano, M., Villagrasa, M., & Negrini, S. (2014). Physiotherapeutic scoliosis-specific exercises for adolescents with idiopathic scoliosis. European Journal of Physical and Rehabilitation Medicine, 50(1), 111-121.
- Marchese, R., Du Plessis, J., Pooke, T., & McAviney, J. (2024). The Improvement of Trunk Muscle Endurance in Adolescents with Idiopathic Scoliosis Treated with ScoliBrace® and the ScoliBalance® Exercise Approach. Journal of Clinical Medicine, 13(3), 653. https://doi.org/10.3390/jcm13030653


