
A comprehensive scoliosis screening exam includes an Adam’s forward bend test that looks for indicators of scoliosis while patients maintain a position that makes the spine highly visible. If a screening exam finds indicators of scoliosis, further testing is warranted; a scoliosis X-ray is needed to reach a diagnosis.
An Adam’s forward bend test is a widely-used scoliosis screening tool that involves examining a patient’s spine and trunk while in a forward-bend position; the spine and related asymmetries, such as uneven shoulders and hips, can be highly visible in this position.
Before getting to the specifics of an Adam’s forward bend test, let’s talk about the importance of regular scoliosis screening.
Scoliosis Screening
There are never treatment guarantees, but we know the sooner treatment is started, the better.
As a progressive condition that’s triggered by growth, the nature of scoliosis is to increase over time, and this means the size and rotation of the sideways-bending and rotating spinal curve is becoming more severe (1).
Progression makes a condition more complex to treat; minor curves are easier to correct than large curves, and while the body can make a number of compensations, when it comes to postural changes, they become harder to improve and/or reverse the longer they’re established (1).
Scoliosis that’s left untreated is likely to become more severe over time, and the more severe, the higher the risk of potential complications.
Scoliosis screening involves looking for early signs of scoliosis with the goal of early detection and intervention, and if risk factors are present, screening from an early age is recommended (2).
Scoliosis affects all ages, but is most commonly diagnosed in children, and as progression is triggered by growth, young patients may face a significant amount of progression (1).
The most prevalent form of scoliosis overall is adolescent idiopathic scoliosis diagnosed around the age of 11 or 12 in females, and a little later in males, and this age group is also the most at risk for rapid advancement due to the stage of growth they are in (2).

Assessment
If there’s concern that a child is showing signs of scoliosis and/or there are risk factors present, an assessment is needed (2).
ScoliCare Clinics are patient-centered, and an experienced team of Clinicians will work towards securing the best possible treatment outcome for every patient,
and this starts with a comprehensive initial assessment.
A patient’s initial assessment and scoliosis X-ray informs the crafting of treatment plans, so it’s crucial that they are as comprehensive and accurate as possible.
An initial assessment can include taking a patient’s medical and family history, postural, movement, and standing assessments, and an Adam’s forward bend test (2, 3).
A patient’s medical history focuses on spinal health, and a family history of scoliosis is considered a primary risk factor; for patients with another sibling or family member diagnosed with scoliosis, this increases the likelihood of another diagnosis (2, 3, 4).
Additional risk factors include gender and age. Females are diagnosed earlier and tend to progress faster than males, and as scoliosis most often appears during adolescence, female adolescents with a family history of scoliosis are the most at risk and are recommended to have regular screening tests (2, 4).
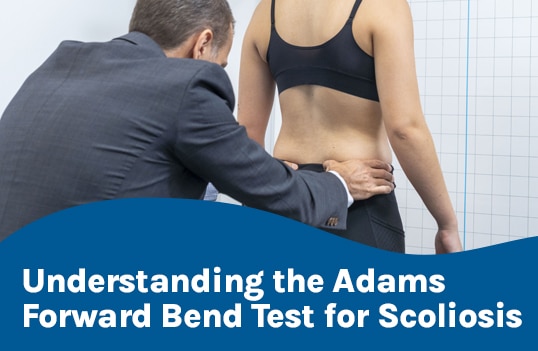
Adam’s Forward Bend Test
An Adam’s forward bend test involves having a patient bend forward as if trying to touch the toes; they remain in this forward-bend position while the spine and trunk are examined (3).
In a forward-bend position, the spine is highly visible, and in most cases, the earliest signs of scoliosis involve postural changes such as uneven shoulders, uneven hips, and a rib cage arch, and these asymmetries are also highly visible in this position (2, 3).
A scoliometer reading can also be applied to indicate a patient’s angle of trunk rotation (ATR). To be considered a true scoliosis, the spine has to bend to the side and rotate, making it a 3-dimensional condition (3).
So if a patient’s initial assessment has found enough indicators of scoliosis to warrant further testing, the next step is a scoliosis X-ray.
Scoliosis X-Ray
What patients need to understand about an Adams forward bend test, and/or scoliosis screening tests in general, is that they can’t diagnose a scoliosis; an X-ray is needed to diagnose and further assess scoliosis through a number of precise curvature measurements.
Scoliosis involves the spine rotating, in addition to unnaturally bending to the side, and the curve size has to be a minimum of 10 degrees, determined by a patient’s Cobb angle measurement (1, 2).
As a progressive condition, we know curve size is likely to change, and as this initial measurement determines severity, it’s one that’s referred back to regularly throughout the course of treatment to determine how the spine is responding to treatment and/or growth; its accuracy is important (5).
A patient’s Cobb angle determines the degree of scoliosis, and an X-ray can also determine a patient’s angle of trunk rotation, the main spinal section affected, how the spine’s surroundings are affected, curve type, and bone age (6, 7).
A patient’s bone age is important because as progression is triggered by growth, estimating how much growth is remaining before a patient reaches skeletal maturity can help craft a strategy for managing/counteracting progression (6, 7).
The more information there is about a patient’s scoliosis, and the more accurate the information is, the less limitations there are to nonsurgical treatment.
So if a patient’s Adam’s bend test has shown indicators of scoliosis and X-ray imaging shows an unnatural lateral spinal curvature of more than 10 degrees with rotation, a diagnosis of scoliosis is reached.
Following a diagnosis, the most important decision is how to respond with treatment.
Scoliosis Treatment Options
A patient’s initial assessment looks for indicators of scoliosis and identifies risk factors; the next step is a scoliosis X-ray.
If a diagnosis is reached, it’s time to start treatment. Remember, as a progressive condition, it’s unlikely that scoliosis won’t progress, particularly when it comes to growth-triggered progression (1).
While scoliosis surgery remains a treatment option, it is invasive, and many patients respond to a proactive approach combining multiple nonsurgical treatment options.
ScoliCare Clinics around the world offer an evidence-based nonsurgical treatment approach that customizes treatment plans to include scoliosis-specific exercise, and corrective bracing.
ScoliBalance® is an innovative program that integrates the principles of Chiropractic BioPhysics® with what established physical therapy programs like the Scientific Exercises Approach to Scoliosis (SEAS) and the Schroth Method have to offer (7, 8, 9). It harnesses the best principles and concepts of multiple methods to create an individualized approach for every patient, acknowledging that no one way fits all patients (10, 11)
Through combining the power of scoliosis-specific chiropractic care and scoliosis-specific exercise, the spine’s alignment may be significantly improved, along with the spine’s surrounding muscle strength for more spinal support and stability (7, 8).
As patients are taught to perform the exercises correctly, they are also taught postural awareness by performing them in front of mirrors; knowing how to position the body and spine during daily activity is important for improving trunk muscle endurance and sustaining treatment results (12).
When a corrective brace like the ScoliBrace® is also applied, the spine’s position can be further improved as it’s held in an overcorrective position, and as the ScoliBrace® is designed with movement in mind, it complements scoliosis-specific exercise-based treatment for the best results.
Conclusion
An Adam’s forward bend test is a standard scoliosis screening examination that looks for indicators of scoliosis.
An Adam’s test involves patients having their spines and torsos examined while in a forward-bend position, making the spine and related trunk asymmetries more noticeable.
What’s important to understand about an Adam’s test is that it can’t diagnose scoliosis; a scoliosis X-ray that confirms the size and rotation of the unnatural spinal curvature is needed.
What an Adam’s test can do is identify noticeable postural changes including uneven shoulders, hips, a characteristic rib arch, and the need for further testing.
If risk factors such as age, gender, and a family history are present, regular and early screening is recommended; managing childhood scoliosis through growth is key.
Significant progression may be preventable with a proactive treatment approach that values early detection and intervention.
References:
- Weinstein, S. L. (2019). The natural history of adolescent idiopathic scoliosis. Journal of Pediatric Orthopaedics, 39, S44-S46.
- Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, Diers H, Grivas TB, Knott P, Kotwicki T, Lebel A, Marti C, Maruyama T, O’Brien J, Price N, Parent E, Rigo M, Romano M, Stikeleather L, Wynne J, Zaina F. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018 Jan 10;13:3. doi: 10.1186/s13013-017-0145-8. PMID: 29435499; PMCID: PMC5795289
- Dunn J, Henrikson NB, Morrison CC, et al. Screening for Adolescent Idiopathic Scoliosis: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Jan. (Evidence Synthesis, No. 156.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK493367/
- Côté P, Kreitz BG, Cassidy JD, Dzus AK, Martel J. A study of the diagnostic accuracy and reliability of the Scoliometer and Adam’s forward bend test. Spine (Phila Pa 1976). 1998 Apr 1;23(7):796-802; discussion 803. doi: 10.1097/00007632-199804010-00011. PMID: 9563110
- Scaturro D, Costantino C, Terrana P, Vitagliani F, Falco V, Cuntrera D, Sannasardo CE, Vitale F, Letizia Mauro G. Risk Factors, Lifestyle and Prevention among Adolescents with Idiopathic Juvenile Scoliosis: A Cross Sectional Study in Eleven First-Grade Secondary Schools of Palermo Province, Italy. Int J Environ Res Public Health. 2021 Nov 24;18(23):12335. doi: 10.3390/ijerph182312335. PMID: 34886069; PMCID: PMC8656498
- Wang, J., Zhang, J., Xu, R. et al. Measurement of scoliosis Cobb angle by end vertebra tilt angle method. J Orthop Surg Res 13, 223 (2018). https://doi.org/10.1186/s13018-018-0928-5
- Dhar S, Dangerfield PH, Dorgan JC, Klenerman L. Correlation between bone age and Risser’s sign in adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 1993 Jan;18(1):14-9. doi: 10.1097/00007632-199301000-00003. PMID: 8434315
- Oakley PA, Harrison DD, Harrison DE, Haas JW. Evidence-based protocol for structural rehabilitation of the spine and posture: review of clinical biomechanics of posture (CBP) publications. J Can Chiropr Assoc. 2005 Dec;49(4):270-96. PMID: 17549209; PMCID: PMC1840024
- Berdishevsky, H., Lebel, V.A., Bettany-Saltikov, J. et al. Physiotherapy scoliosis-specific exercises – a comprehensive review of seven major schools. Scoliosis 11, 20 (2016). https://doi.org/10.1186/s13013-016-0076-9
- Marchese, R. (2023). World-wide variation in Schroth therapists’ clinical reasoning and exercise prescription for adolescents with idiopathic scoliosis (Doctoral dissertation, Macquarie University).
- Marchese, R., Ilhan, E., & Pacey, V. (2023). How Schroth therapists vary the implementation of Schroth worldwide for adolescents with idiopathic scoliosis: a mixed methods study. Journal of Clinical Medicine, 12(18), 6063.
- Marchese, R., Du Plessis, J., Pooke, T., & McAviney, J. (2024). The improvement of trunk muscle endurance in adolescents with idiopathic scoliosis treated with ScoliBrace® and the ScoliBalance® exercise approach. Journal of Clinical Medicine, 13(3), 653.
More news
-
 8 August 2024
8 August 2024Receiving a scoliosis diagnosis often brings a flood of questions and concerns about the future. How did this happen? What are the scoliosis treatment options? Is scoliosis surgery necessary? Navigating…
-
 17 July 2024
17 July 2024Receiving a scoliosis diagnosis as an adult can be daunting. Many people wonder how it happened, what the future holds, and whether it can be treated. Understanding scoliosis in adults…
-
 14 March 2021
14 March 2021Kurt Cobain and his Scoliosis Part of our series of famous people who have/had a Scoliosis. Next up is Kurt Cobain! Kurt Cobain is best known as the lead…