Why ‘Wait and See’ is Not a Treatment Option for Scoliosis
Written by Rose Mirenzi
Last Updated:
› News › Why ‘Wait and See’ is Not a Treatment Option for Scoliosis
Why ‘Wait and See’ is Not a Treatment Option for Scoliosis
The ‘wait and see’ approach to scoliosis is not a treatment option or healing strategy. Despite growing evidence and international guidelines (1, 2, 3, 4, 5) to support conservative treatment options for scoliosis, unfortunately some patients are still told to ‘do nothing’ unless the scoliosis progresses to the point of needing surgery.
When there are options for patients, and timely treatment is so important (4, 5), patients must be given the option for conservative care where possible. Why should you not let them ‘wait and see’?
Scoliosis Progression Risk is Highest During Growth Spurts
It is so important that patients (and their caregivers) are given the option to receive conservative treatment care (structured observation, scoliosis specific exercises and/or bracing) while it can be most effective (2). This is particularly important in very young children with juvenile idiopathic scoliosis (JIS) and adolescents with idiopathic scoliosis (AIS). Progression and increased structural and postural damage is highest often during the growth spurts. Don’t let the patients miss out on their options!
Patients Deserve to be Empowered with Choice
If there are treatment options available for patients, and there are, then the patients have the right to be informed of such choices. It’s also not just the Cobb angle we are concerned with when treating these patients (6). Patients with scoliosis also have the right to decide if conservative treatment options are worth pursuing in order to help them with additional goals such as improving aesthetics (6).
It can Often Lead to Surgery
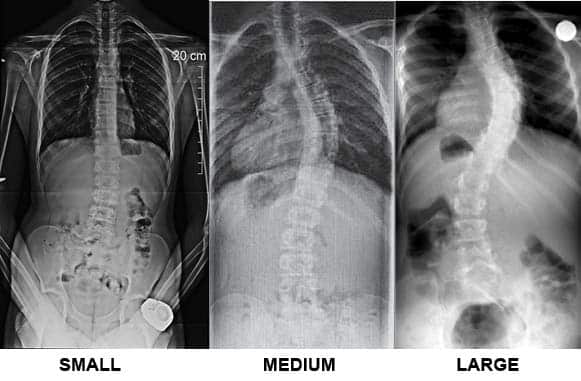
This is a massive problem, particularly with the younger patients with JIS (7). Young children with JIS have a very high risk of progression (7). In fact, when it’s a child with JIS and a Cobb angle greater than 30 degrees will have a 100% prognosis for surgery whereby the curve progresses to 40-45 degrees (7). While progression risk is a little harder to predict with curves between 21 and 30 degrees during the first two years of puberty we are still becoming more certain every day that these kids may benefit from a treatment regime of scoliosis specific exercises and bracing (4, 5). If the curves are caught early enough, some patients may even be able to trial a course of scoliosis specific exercises without the bracing. However, once the curves get to 20-25 degrees (possibly earlier in the very young) it is imperative that they are given the option of a combined treatment approach (bracing and scoliosis specific exercises) (2).
Remember kids with scoliosis will eventually be adults with scoliosis. Missing out on early treatment options really does lead to a missed opportunity to empower these patients with choice. There is no cure for scoliosis so the sooner they are educated about the condition the better. Each patient deserves a holistic approach. The Cobb angle is one part, not the entire story (6).
References:
Monticone, M., Ambrosini, E., Cazzaniga, D., Rocca, B, and Ferrante, S. (2014). Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial. Euro Spine J 23: 1204-1214.
Negrini, S., Donzelli, S., Aulisa, A. G., Czaprowski, D., Schreiber, S., de Mauroy, J. C., Zaina, F. (2018). 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord, 13(1), 3-3. doi:10.1186/s13013-017-0145-8
Negrini, A., Negrini, MG., Donzelli, S., Romano, M., Zaina, F. and Negrini, S. (2015). Scoliosis-specific exercises can reduce the progression of severe curves in adult idiopathic scoliosis: a long-term cohort study. Scoliosis 10: 20.
Zhour, Z., Liu, F., Li, R. and Chen X. (2021). The effects of exercise therapy on adolescent idiopathic scoliosis: An overview of systematic review and meta-analyses.
Weinstein, S., Dolan, LA., Wright, JG., and Dobbs, MB. (2013). Effects of bracing in adolescents with idiopathic scoliosis. The New England Journal of Medicine. 369: 1512-1521.
Negrini, S., Grivas, T., Kotwicki, T., Maruyama, T., Rigo, M., Weiss, HR., SOSORT members (2006). Why do we treat adolescent idiopathic scoliosis? What we want to obtain and avoid for our patients. SOSORT 2005 Consensus paper. Scoliosis (2006) 1: 4.
Charles, YP., Daures, JP., de Rosa, V., and Demeglio, A. (2006). Progression risk of idiopathic juvenile scoliosis during pubertal growth. Spine (Phila Pa 1976) 1: 31 (17):1933-42.
Chief of Research and Communications, Physiotherapist
Rose manages education, training and research at ScoliCare, is a physiotherapist, speaker, educator, and writer, and has extensive experience in assessing and treating patients with scoliosis. Rose has been instrumental in further developing the ScoliBalance concept created over many years by ScoliCare's CEO, Dr. Jeb McAviney.
In recent years, patient-centred care has revolutionised the approach to scoliosis treatment by focusing on the unique needs, preferences and values of each patient. This approach places patients at the…
Kurt Cobain and his Scoliosis Part of our series of famous people who have/had a Scoliosis. Next up is Kurt Cobain! Kurt Cobain is best known as the lead…
It is hard to believe that the fastest man on earth has scoliosis! Olympian Usain Bolt was born with scoliosis. His right leg is half an inch shorter than his…
This website uses tracking cookies and third party services. To learn how this information is stored and used, please visit the Privacy Policy and Terms & Conditions pages


 15 July 2024
15 July 2024 14 March 2021
14 March 2021 1 November 2022
1 November 2022