
Scoliosis is often thought of as a condition of a young child or teenager. You may even find that some of your patients who were not diagnosed with scoliosis as a child are surprised by a new diagnosis of scoliosis in adulthood. There is no cure for scoliosis – your patient will always have scoliosis. So, can scoliosis in adults be ‘treated’? Well, it depends how ‘treatment’ is defined. Is the aim to reduce Cobb angle? Reduce pain? Improve posture? Minimise or halt progression? There are various potential goals for each patient.
Your job is to recognise the different types, and treatment considerations, to best suit your patient. If the goal is to reduce Cobb angle significantly then surgery may indeed be suitable for that patient. However, for other patients conservative options will serve them much better.

Adult Scoliosis Needs Attention
Remember scoliosis that starts in the teen years can go unnoticed. So when you see an adult patient that is newly diagnosed with scoliosis, you may well be seeing an idiopathic scoliosis situation from teen years.
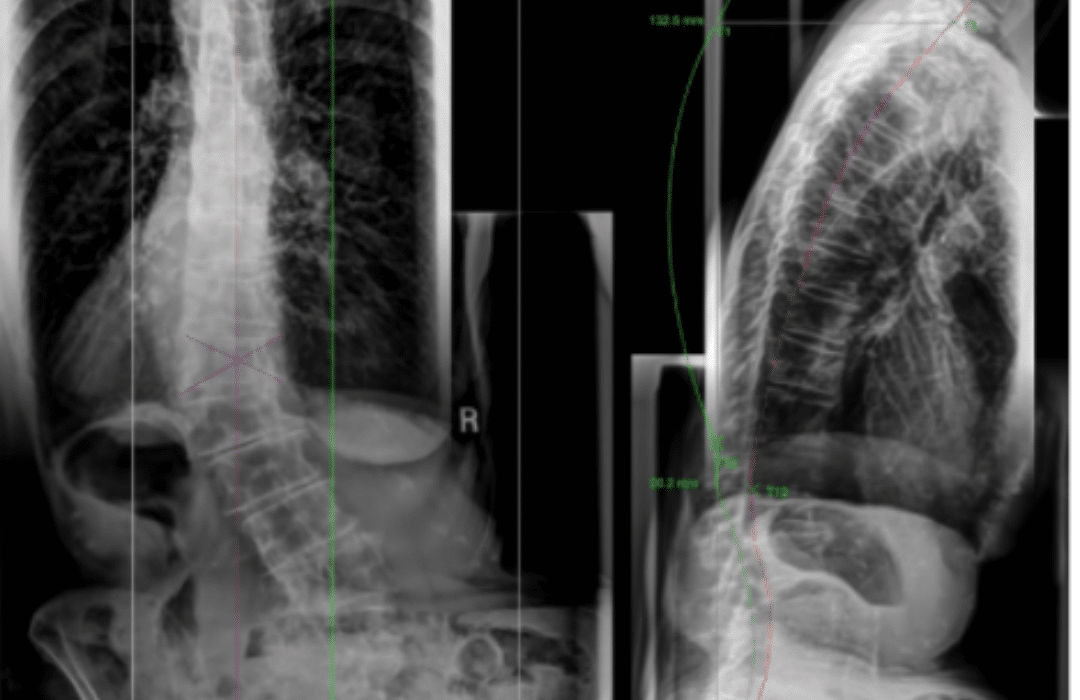
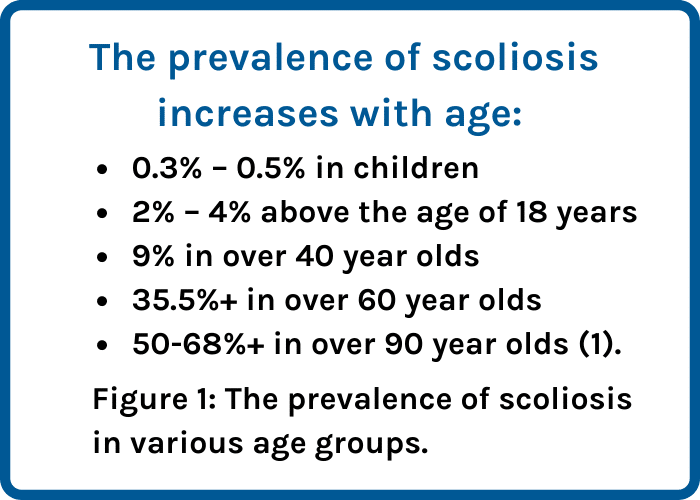
In the clinic there is often a large focus on adolescents with idiopathic scoliosis. This type of scoliosis requires attention to avoid progression during the high risk phase of puberty. So this raises the question; are adults with scoliosis getting enough attention? We have an ageing population and it’s quite clear that the prevalence of scoliosis increases with age (Figure 1).
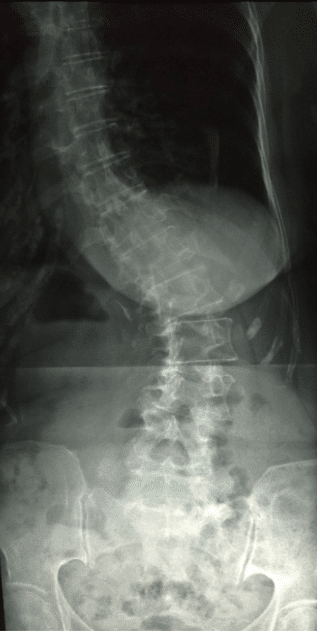
There are various types of scoliosis in adults. Primary (de novo) degenerative scoliosis and secondary degenerative scoliosis are most common in adult patients who present clinically (1).
Figure 2: Adult Degenerative Scoliosis
Conservative treatment for adults with scoliosis
Unlike progression of scoliosis in adolescents, progression of adult scoliosis revolves around degenerative instability as opposed to growth modulation.
Problems associated with adult spinal deformity include:
-
-
-
-
-
-
- Pain
- Disability
- Progression
- Aesthetics
-
-
-
-
-
In adult treatment it is important to realise that both the natural history and the goals of treatment are very different compared to treatment for adolescents. In adolescents, scoliosis is generally more highly progressive, pain is not an overriding issue but can occur, and the curves are often flexible. Correction or stabilisation are the primary goals.
In adults the curves are generally slowly progressive (with the exception of some types of scoliosis). Pain is usually the main issue. The curves are usually rigid and therefore only a limited amount of Cobb angle correction can be achieved, if any at all (2, 3).
Physiotherapeutic scoliosis specific exercises (PSSE) are recommended in the treatment of adolescents with idiopathic scoliosis according to international guidelines (4). The evidence in support of such exercise continues to grow.
On the flipside, there is definitely less research that has investigated the use of PSSE or bracing for adults, however the evidence that does exist is positive.
Palazzo and colleagues (2017) and Negrini and colleagues (2015) showed support for the use of bracing and scoliosis specific exercises respectively for the treatment of adults with scoliosis (5, 6).
Scoliosis specific exercises and bracing may be a suitable option for your adult patients with scoliosis.
We definitely need more research in this area, however recruiting patients may be somewhat difficult. Adults who seek treatment will often be in pain and will not likely opt for a ‘no treatment’ approach, making randomised controlled trials challenging. For now, clinical experience and discussions with colleagues from around the world will likely quickly show you that there is a demand for conservative treatment options for adults with scoliosis, and these patients deserve the chance to discuss their options.
References:
- Berven, SH. and Lowe, T. (2007) The Scoliosis Research Society classification for adult spinal deformity. Neurosurg Clin North Am 18(2):207–213.
- Schwab, F; Dubey, A., Gamez, L. El Fegoun, AB., Hwang, K.,Pagala, M., Farcy, JP. (2005). Adult Scoliosis: Prevalence, SF-36, and Nutritional Parameters in an Elderly Volunteer Population, Spine: May 1, 2005 – Volume 30 – Issue 9 – p 1082-1085 doi: 10.1097/01.brs.0000160842.43482.cd
- McAviney, J. Mee, J. Fazalbhoy, A. Du Plessis, J. Brown, BT. (2020). A systematic literature review of spinal brace/orthosis treatment for adults with scoliosis between 1967 and 2018: clinical outcomes and harms data. BMC Musculoskelet Disord. 21(1):87. doi: 10.1186/s12891-020-3095-x. PMID: 32035480; PMCID: PMC7007692.
- Negrini, S., Donzelli, S., Aulisa, A.G. et al. (2018). 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis 13, 3 . https://doi.org/10.
- Palazzo, C., Montigny, JP., Barbot, F., Bustle, B., Vaugier, I., Fort, D., Courtois, I., and Marty-Poumarat, C. (2017). Effects of bracing in adults with scoliosis: A retrospective cohort study. Archives of Physical Medicine and Rehabilitation. 98: 187-190.
- Negrini, A., Negrini, M.G., Donzelli, S. et al. (2015). Scoliosis-Specific exercises can reduce the progression of severe curves in adult idiopathic scoliosis: a long-term cohort study. Scoliosis 10, 20.https://doi.org/10.1186/s13013-015-0044-9

More news
-
 17 July 2024
17 July 2024Receiving a scoliosis diagnosis as an adult can be daunting. Many people wonder how it happened, what the future holds, and whether it can be treated. Understanding scoliosis in adults…
-
 8 August 2024
8 August 2024Receiving a scoliosis diagnosis often brings a flood of questions and concerns about the future. How did this happen? What are the scoliosis treatment options? Is scoliosis surgery necessary? Navigating…
-
 25 October 2023
25 October 2023Back pain in patients with scoliosis is quite prevalent. It is also possible that patients with scoliosis present with specific features of low back or leg pain. ScoliCare Head of…