

The prevalence of adults with idiopathic scoliosis is likely to increase with the ageing population considering humans are generally living longer. Scoliosis fusion surgery is generally considered the primary, if not only, approach for stopping progression of the curve in these patients. Long term follow up of adolescents with idiopathic scoliosis has shown that the scoliosis can progress during adulthood even after skeletal maturity has been reached [1]. Despite the lack of the fast growth period that accompanies progression risk for adolescents, adults with idiopathic scoliosis also face progression risk. Asymmetric loading, with or without any developing degeneration, increases the progression of the curve and accompanying deformity [2]. There are, however, some patients who refuse surgery. These patients in particular, need conservative treatment options that may help them achieve their goals. This is especially important considering that 60% of these cases progress, especially if the curve exceeds 30 degrees at skeletal maturity [3, 4].
How can Scoliosis Specific Exercises Help Adults with Idiopathic Scoliosis?
Scoliosis specific exercises have been shown to be superior to natural history in adults with idiopathic scoliosis [5]. The results from a cohort study showed that scoliosis specific exercises can be effective to obtain stability and in some cases reduce the Cobb angle in degrees . In highly progressive cases the authors showed that the curve worsening can be slowed [5]. The authors also emphasised that continuity and consistency of performing the exercises is essential to minimise any loss of gains [5].
Scoliosis is composed of postural, elastic, and structural components. While the literature often describes the structural deformity of the spine, it is important to remember that there are elastic changes that also occur, which affect posture. The patients are also affected by the impacts of trying to hold their posture in an upright position. In adults with idiopathic scoliosis, particularly if degeneration kicks in, this may be particularly difficult.
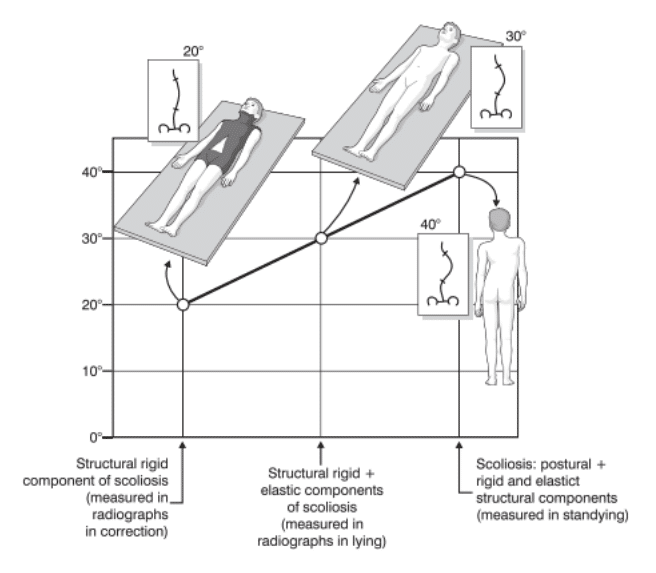
Adults with idiopathic scoliosis with Cobb angles greater than 60 degrees, that perform an X-ray at different times of the day, will see a measurement error whereby the curve appears worse later in the day [6]. This is due to the postural collapse of the spine. We can also see scoliosis curves ‘improve’ when comparing Cobb angles in standing compared to lying down. When lying down, the postural collapse is somewhat removed and the measurements taken are a result of the elastic and structural components of scoliosis. This was described by Duval-Beaupere and can be seen in the image below. The patient on the left is wearing a cast in supine, the patient in the middle is supine without a cast, and the patient on the right is standing without a cast. You can see the scoliosis is worse in the latter two images. Scoliosis specific exercises are aimed at addressing the postural components of the scoliosis. In adults this is particularly important as the day goes on and the effects of gravity and postural collapse take place [7, 8].
Implementing Scoliosis Specific Exercises in Adults with Idiopathic Scoliosis
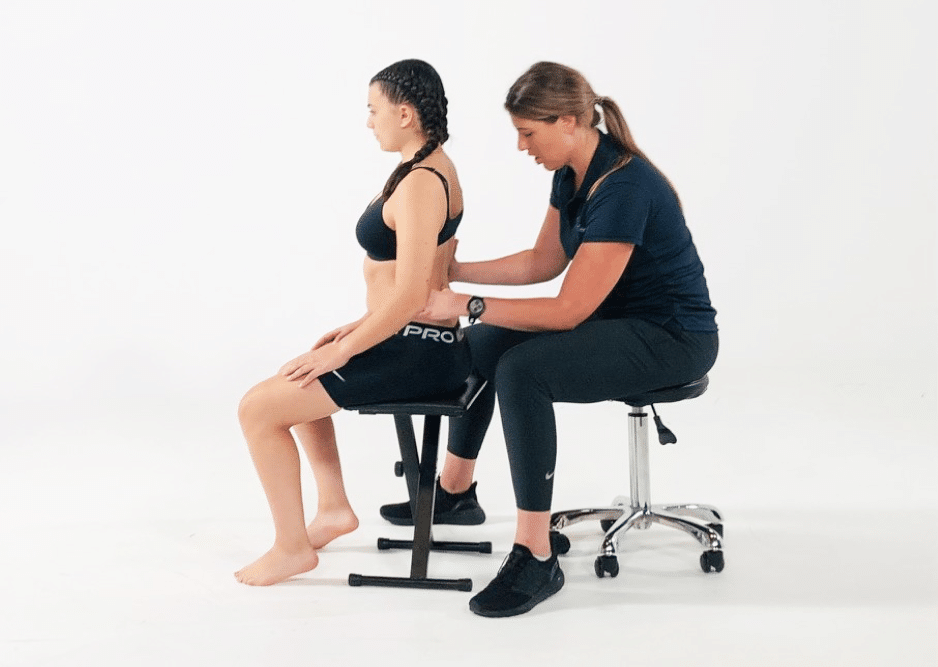
Scoliosis specific exercises for adults can be a valuable component of the management of their scoliosis. It is important that the exercise program is designed and delivered by a health professional specifically trained and certified in scoliosis specific exercise protocols. The program should be individualised and not just a generic exercise program. Adults can usually continue with many of their usual exercise pursuits, but a health professional specifically trained in scoliosis specific rehabilitation will also be able to provide some guidance on the pros and cons of their general exercise pursuits.
ScoliBalance Providers can be found in Australia and internationally on this directory.
References:
- Collis D, Ponseti IV. (1969) Long-term follow-up of patients with idiopathic scoliosis not treated surgically. J Bone Joint Surg AM 51:425-445
- Aebi M (2005) The adult scoliosis. European spine journal 14:925-948. doi: 10.1007/s00586-005-1053-9
- Weinstein SL (1999) Natural history Spine 24:2592-2600
- Weinstein SL, Dolan LA, Spratt KF, Peterson KK, Spoonamore MJ, Ponseti IV (2003) Health and Function of Patients With Untreated Idiopathic Scoliosis: A 50-Year Natural History Study. JAMA : the journal of the American Medical Association 289:559-567. doi: 10.1001/jama.289.5.559
- Negrini A, Negrini MG, Donzelli S, Romano M, Zaina F, Negrini S (2015) Scoliosis-Specific exercises can reduce the progression of severe curves in adult idiopathic scoliosis: a long-term cohort study. Scoliosis 10:20. doi: 10.1186/s13013-015-0044-9
- Stokes IAF, Burwell RG, Dangerfield PH (2006) Biomechanical spinal growth modulation and progressive adolescent scoliosis – A test of the ‘vicious cycle’ pathogenetic hypothesis: Summary of an electronic focus group debate of the IBSE. Scoliosis 1:16-16. doi: 10.1186/1748-7161-1-16
- Duval-Beaupère G, Lespargot, A. and Grossord (1985) Flexibility of scoliosis. What does it mean? Is this terminology appropriate? Spine (Phila Pa 1976) 10:428-432
- Duval-Beaupere G (1996) Threshold values for supine and standing Cobb angles and rib hump measurements: Prognostic factors for scoliosis. European spine journal 5:79-84. doi: 10.1007/BF00298385

More news
-
 19 October 2021
19 October 2021This month we take you behind the scenes of the treatment story of a 14 year old girl with adolescent idiopathic scoliosis who opted for a ScoliBrace. Let’s call her…
-
 26 August 2021
26 August 2021The potential effectiveness of scoliosis specific exercises can at times create much debate. This was particularly evident in the past when scientific evidence in support of such therapy was limited…
-
 12 January 2022
12 January 2022Juvenile idiopathic scoliosis (JIS) needs careful attention and it is so important that these children are not ‘missed’. With much of the attention in the literature often falling to the…