63 year old female patient with progressive idiopathic scoliosis into adulthood.
Postural and curve improvement in an adult female patient with scoliosis using ScoliBrace and ScoliBalance
Summary:
This case demonstrates the successful management of a patient with progressive idiopathic scoliosis into adulthood. The patient presented with significant postural concerns, and fear of her scoliosis progressing further. The patient did not present with pain. The patient had a 32° right thoracic curve and a 19° left lumbar curve with good coronal balance. There were alterations to the normal lordosis and kyphosis angles. All curve measurements are reported as Cobb angles.
The patient was prescribed a rigid 3D designed custom orthosis (ScoliBrace) to be worn each day on a part-time basis. The patient has been wearing the brace during the day for the past 2 years. Clinical and radiological findings from the most recent follow-up appointment indicate that the patient’s scoliosis has been improved and stabilized. The patient reports that she has more confidence and a better outlook on her future with scoliosis.
Case Background
The 61-year-old female patient was referred to the ScoliCare clinic by her general practitioner. The patient had been diagnosed with scoliosis at 14 years of age and told the measurement was 32°. At that time she was prescribed a Boston Brace to wear full time. She was compliant and wore the brace on average 23 hours per day for the first two years, then at a decreased number until the age of 23. The Cobb angle was reported to be 27°. She discontinued use of the brace.
She reports having been checked at the age of 40 and says the X-rays were ‘satisfactory’. Previous X-rays were not available for review.
At the time she presented to the clinic, she had seen some postural changes including prominent shoulder blade, rib hump, and trunk rotation. Primary concern was curve progression.
Examination Findings
A detailed history and physical examination were performed.
The patient reported no family history of scoliosis or significant medical history or comorbidities. She reported no pain in her activities daily living, but had a positive Kemp’s test on the left side.
The physical examination revealed anterior head translation and good coronal balance in the postural assessment. There was evidence of spinal curvature in the thoracic region along with asymmetries in the waist region (Figure 1).
Physical examination revealed a generalized decrease in the lumbar range of motion with right lumbar lateral flexion markedly reduced. The Adams forward bend test was positive, with an angle of trunk rotation (ATR) measurement of 12 degrees right thoracic using a scoliometer. The patient’s neurological exam was unremarkable.
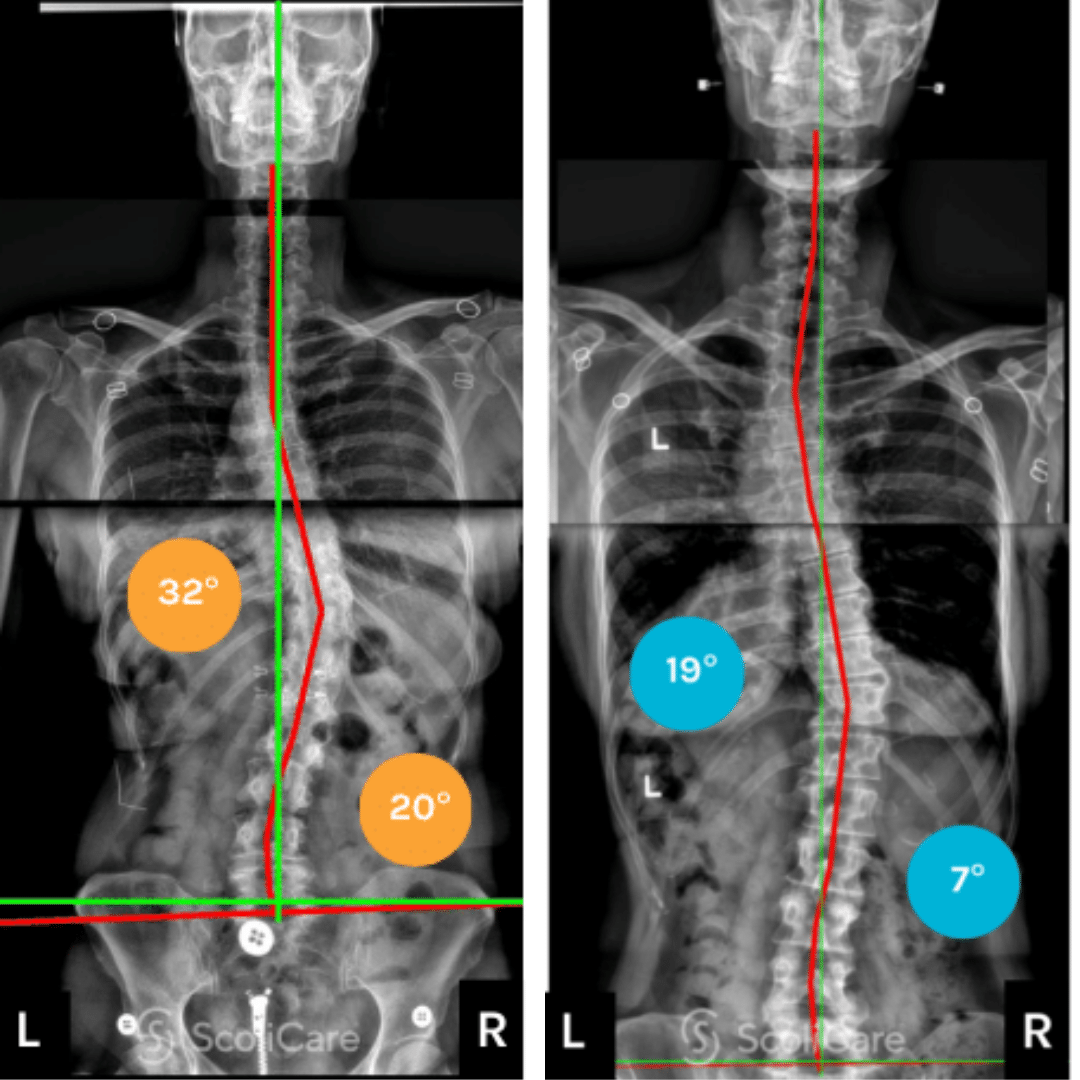
The patient’s X-ray indicated that the scoliosis had progressed from her reported measurements at 40 years old, now measuring 32° in the right thoracic spine and 19° left lumbar spine (Figure 1).
The patient was diagnosed with progressive idiopathic scoliosis into adulthood or ASA (Adolescent Scoliosis in Adults).
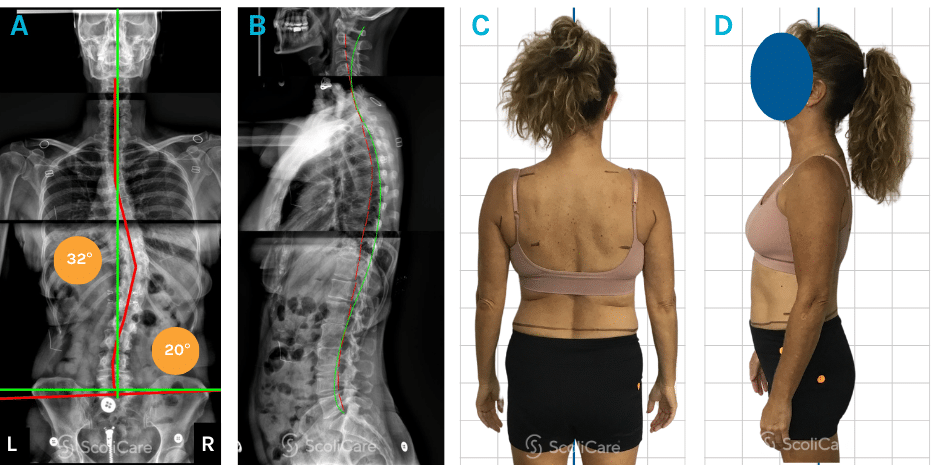
Figure 1: Initial anteroposterior spine X-ray highlighting a 32° right thoracic and 20° left lumbar double curve scoliosis (A). Initial lateral X-ray (B). Posteroanterior postural photograph (C), Lateral postural photograph (D).
Intervention
The patient was prescribed a 3D customized, rigid orthosis (ScoliBrace) designed to correct and stabilize the deformity in the thoracic and lumbar spine. The brace was fitted three months after the initial consultation. The patient was advised to wear the brace initially for one to two hours each day then increase the wear by half to one hour each day up to a level that was tolerable. The minimum recommended hours for the patient was 8 hours.
The patient was also enrolled in ScoliBalance. This scoliosis specific rehabilitation program was prescribed to help stabilize the curve and complement the brace. The 3D active self-corrections (ScoliCorrections) prescribed to the patient were specific to her scoliosis, and specific exercises (ScoliExercises) were also prescribed to stabilize the corrected posture in 3D and improve core strength and stability.
In-brace photos taken at the time of the brace fitting demonstrated the intended over correction in the patient’s posture. In-brace X-rays were taken 6 weeks after the brace fitting appointment, which demonstrated a reduction in the patient’s scoliosis (Figure 2).
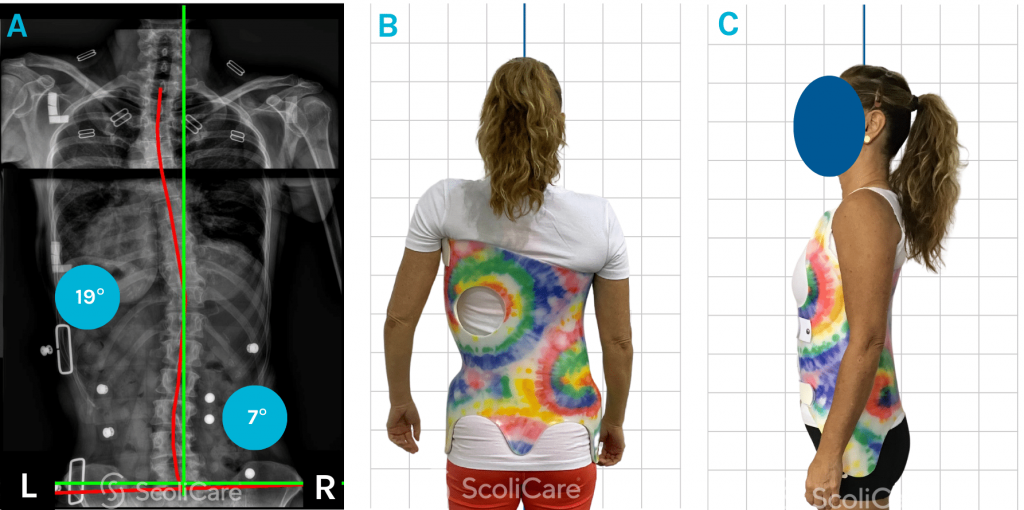
Figure 2: Anteroposterior in-brace X-ray with a 19° right thoracic curve and 7° left lumbar curve. Posteroanterior postural photograph in brace (A). Posteroanterior postural photograph in brace (B). Lateral postural photograph in brace (C)
Outcomes
The patient attended a follow-up consultation six weeks after the brace fitting. The patient reported that overall they were feeling ‘taller’ and ‘straighter’. The patient was able to wear the brace at least 8 hours per day, none of which was done while sleeping. The patient was reviewed again three months later. At this time, the patient stated that they were still able to wear their brace 8 hours per day. The patient had attended 12 ScoliBalance sessions. A decrease was seen in the spinal curvature in the thoracic region in the out-of-brace photos. The patient’s thoracic and lumbar double curve scoliosis had improved to 24° right thoracic curve and 13° left lumbar curve (Figure 3).
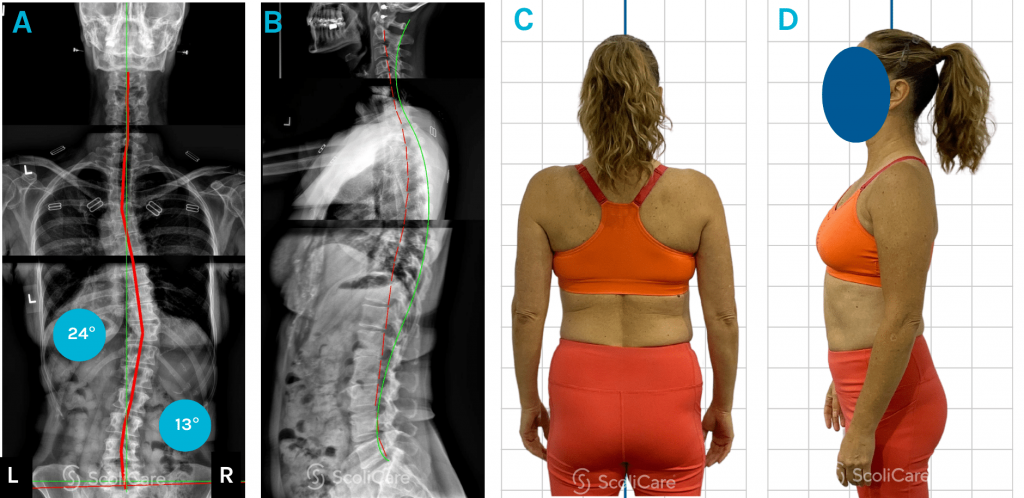
Figure 3: Anteroposterior x-ray with a 24° right thoracic curve and 13° left lumbar curve. (A). Lateral X-ray (B). Posteroanterior postural photograph out-of-brace (C). Lateral postural photograph out-of-brace (D).
At the patient’s two year follow up, she reported wearing the brace on average of 3 hours per day. On examination, it was found that her ATR had decreased and was 5° in the thoracic spine. ATR was negative in the lumbar spine. Upon x-ray review, improvement was seen in the patient’s scoliosis. The patient’s thoracic scoliosis was reduced to 19° and the lumbar was stable at 7° (Figure 4). This was a demonstrated improvement of 41% in the right thoracic curve and 65% in the left lumbar curve. There was a decrease in the patient’s thoracic curve at this time, but it was attributed to the improvement in scoliosis curves.
The patient is still under care and has been advised to continue with bracing during the day for maintenance. They will continue doing ScoliBalance at home and seeing the ScoliBalance Rehabilitation Provider for review and update of the ScoliCorrections and ScoliExercises. The ScoliBalance program will be adjusted to the patient’s new X-rays and clinical presentation.
The patient will be reviewed again in one year.
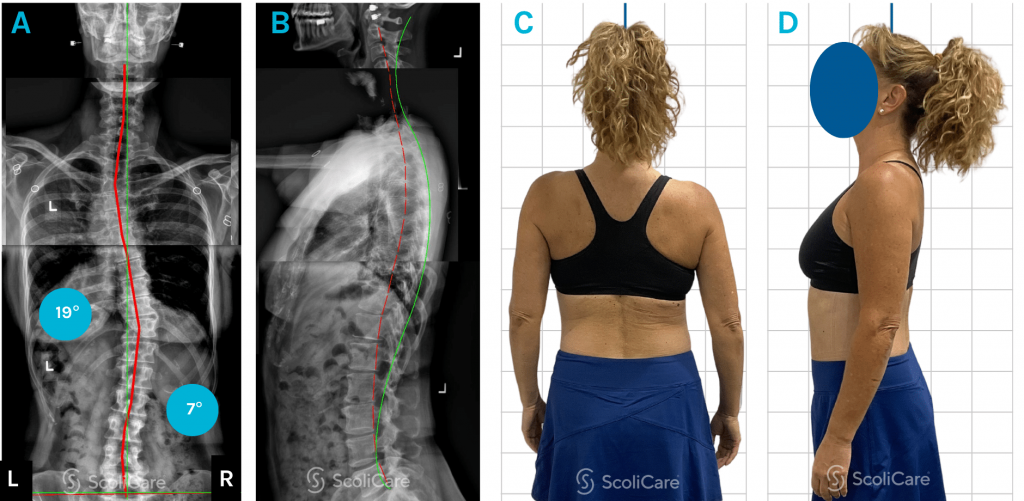
Figure 4: Anteroposterior x-ray with a 19° right thoracic curve and 7° left lumbar curve. (A). Lateral X-ray (B). Posteroanterior postural photograph out-of-brace (C). Lateral postural photograph out-of-brace (D).
Discussion
The subject of this case study represents a typical ASA (Adolescent Scoliosis in Adults) case presentation. Scoliosis that is detected in adolescence can progress into adulthood. This progression is most pronounced in patients entering adulthood with scoliosis measuring >30° (Cobb).
This patient presented with very few symptoms or pain, but had the foresight to understand that spending time in the scoliotic position would start to affect her quality of life. She had been very active throughout her entire life. ScoliBrace and ScoliBalance (Scoliosis Specific Exercise Rehabilitation) has been used in this case to reduce a double curve scoliosis in a 61 year-old active female.
The patient was compliant with her bracing and rehabilitation. Her above average fitness level provided an opportunity to do more advanced exercises.
Conclusion
This case demonstrates the successful management of a 61-year-old female patient with progressive idiopathic scoliosis into adulthood or ASA (Adolescent Scoliosis in Adults) using ScoliBrace (a rigid 3D designed custom orthosis) and ScoliBalance (scoliosis specific rehabilitation). The patient demonstrated good compliance with the brace and has experienced improvements in posture and scoliosis curves.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patients type and severity of scoliosis.
More news
-
 21 February 2023
21 February 2023Today we know that scoliosis affects approximately 2-4% of adolescents. The treatment of scoliosis has evolved over the years, with various approaches being developed to manage the condition. One of…
-
 18 May 2021
18 May 2021“Having my painting used for a custom brace is one of the most unusual requests I have ever received. I am honoured to have my art offered as a choice for a…