Male patient aged 14 years with a right thoracic curve measured at 49 degrees.
Reduction of a severe scoliosis using a custom 3D over-corrective scoliosis brace and scoliosis specific rehabilitation in a 14-year-old male
Summary:
This case demonstrates the management of a young male athlete with a severe scoliosis using a custom 3D designed scoliosis brace and scoliosis specific rehabilitation. The patient presented to the ScoliCare clinic at age 14 with a 49° right thoracic scoliosis. The patient was prescribed the custom scoliosis orthosis to be worn full-time, and taught scoliosis specific exercises and mobilisation techniques to perform at home.
After 21 months of full-time bracing and rehabilitation, the patient’s scoliosis had been reduced from 49° down to 31°. Follow-up x-rays taken at the end of the brace weaning period revealed that the patient’s scoliosis had remained stable at 31°. The patient is still under care and will continue with the scoliosis specific exercises to maintain the correction that has been achieved.
Case Background
The young male patient had been diagnosed with adolescent idiopathic scoliosis (AIS) by a physiotherapist at age 13 years. At that time, the patient was actively involved with Australian Rules Football (AFL), and was also competing in athletics at a national level.
The patient had a right thoracic curve that had measured 39° at the time of the initial diagnosis. The patient and his parents had consulted with a surgeon who had advised that bracing was the most appropriate treatment given the magnitude of the scoliosis.
However, the surgeon did inform the patient that he may become a candidate for surgery if the scoliosis were to progress.
The patient presented to the ScoliCare Clinic one year later for brace therapy. The patient had continued with his sporting and athletic pursuits. Plain films taken at the time of this consultation revealed the patient was Risser 3 and the scoliosis had progressed a further 10°, measuring 49° (Figure 1).
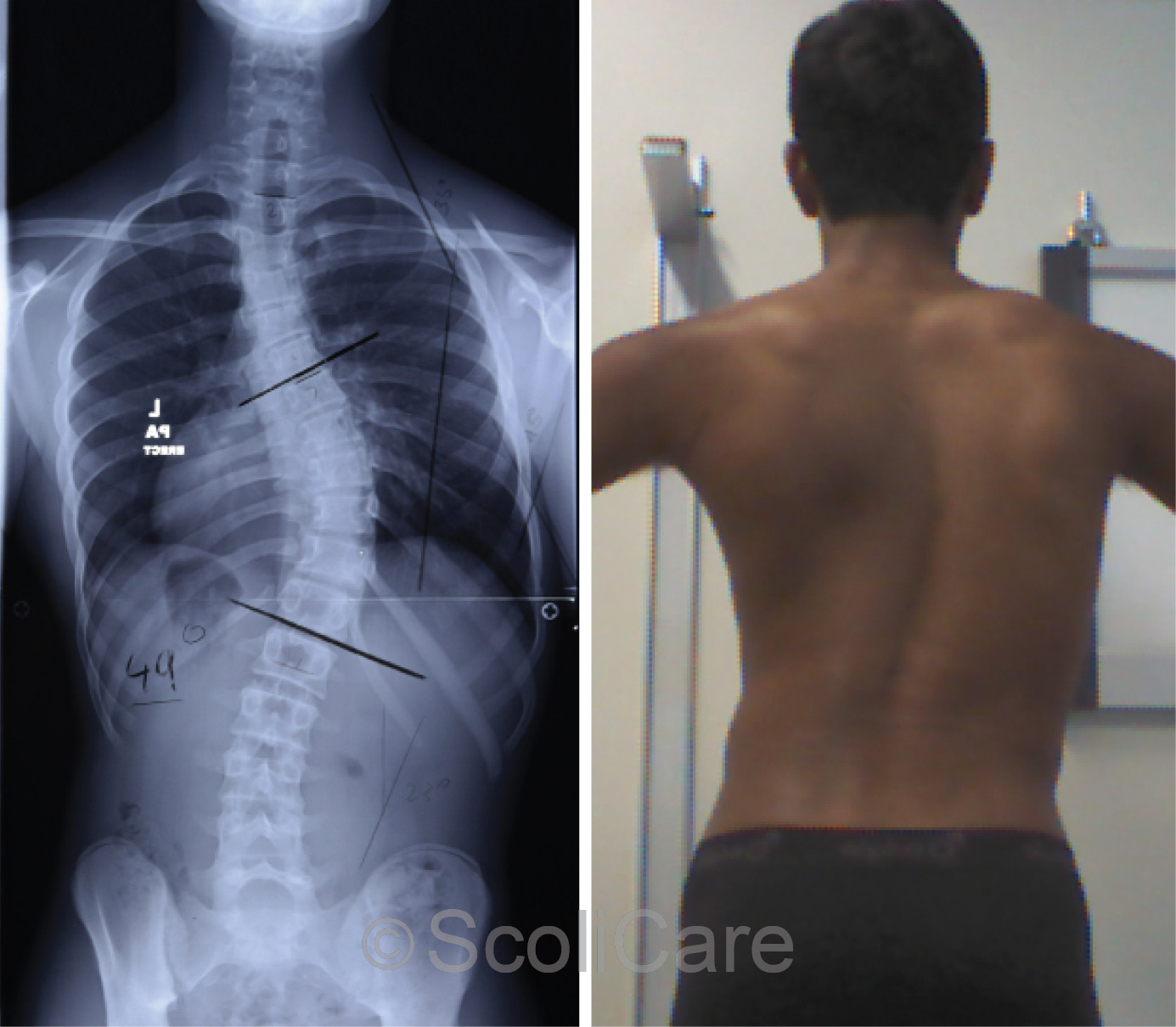
Figure 1: Standing posteroanterior x-ray demonstrating a 49° right thoracic scoliosis (Left),
Standing posteroanterior postural photograph (Right).
Examination Findings
The patient was not experiencing any pain from his scoliosis but was aware of the asymmetrical shape of his torso.
The patient was in good health and the systems review and medical history were unremarkable except that the patient had received grommets as a child for recurrent middle ear infections.
Due to the regular AFL and athletic training, good general strength and flexibility were noted on the physical examination. The patient had an obvious right thoracic curvature with rib humping observed during the Adam’s forward bend test.
No other abnormalities were detected.
Intervention
The patient was prescribed a custom 3D designed scoliosis orthosis, Scientific Exercise Approach to Scoliosis (SEAS) rehabilitation exercises, and home fulcrum-traction using the scoliosis orthotic device.
The patient was required to where the brace for up to 23 hours per day but could take the brace off when training or competing. The patient was instructed to perform the rehabilitation exercises and use the scoliosis orthotic device each day, which in combination, took approximately 40 minutes to complete.
Sport specific exercises were also incorporated into the patient’s program to aid with motivation and to minimise the impact of the rehabilitation program on what was already a busy sporting/athletic schedule.
Outcomes
The patient was a highly motivated young man and his family were very committed to helping him succeed with the treatment. The patient wore the brace and performed the rehabilitation program as prescribed.
Out-of-brace plain films taken approximately 1 year after the initial examination at the ScoliCare clinic highlighted that the patient was Risser 4 and that the scoliosis had been reduced down to 37° (Figure 2).
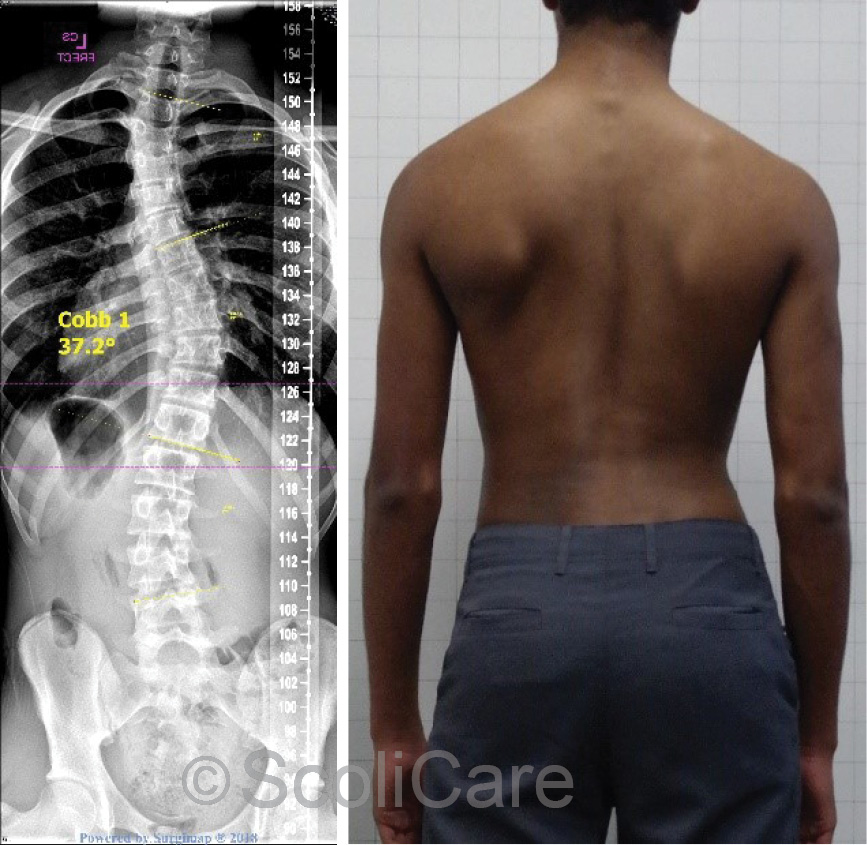
Figure 2: Standing posteroanterior x-ray indicating a right 37° thoracic scoliosis (Left),
Posteroanterior postural photograph (Right)
The patient wore the brace full-time for 21 months in total. Out-of-brace x-rays taken at this time revealed that the patient was now Risser 5 and the scoliosis measured 31° (Figure 3). Brace weaning was initiated from this point, with the patient only wearing the brace after school and at night. At 30 months, brace wear was reduced to night time wear only.
Out-of-brace plain films taken two years and 10 months after the start of bracing demonstrated that the curve had remained stable at 31° (Figure 4). At the most recent follow-up consultation, the patient was performing the rehabilitation exercises 2-3 times per week and continuing with general exercise most days. The angle of trunk rotation at this time measured 7° in the lumbar spine and 6 degrees in the thoracic spine.

Figure 3: Standing posteroanterior x-ray indicating a 31° right thoracic scoliosis (Left),
Posteroanterior postural photograph (Right)
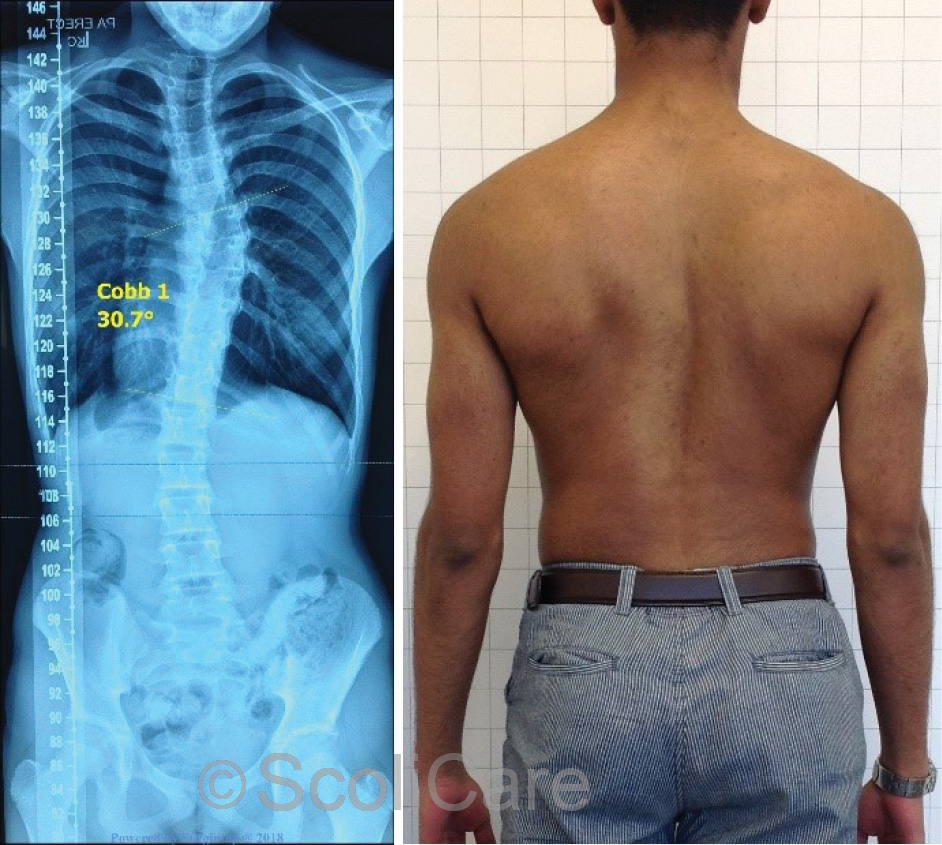
Figure 4: Standing posteroanterior x-ray indicating a 31° right thoracic scoliosis (Left),
Posteroanterior postural photograph (Right)
Discussion
Bracing, SEAS exercises and ScoliRoll fulcrum-traction have been used in this case to significantly reduce a surgical level thoracic curvature in a 14-year-old male. Research has shown that adolescents who are taller, lighter, and thinner have an increased risk of developing scoliosis.
Furthermore, a patient’s muscle mass may be associated with scoliosis, with lower muscle mass contributing to decreased postural strength, control and stability. With reference to somatotype, ectomorphy (versus endo- or mesomorphy) is commonly associated with scoliosis. The patient in this case was competing at a high level in both AFL and athletics.
The muscle mass, strength, flexibility and athleticism that were developed through these physical pursuits have likely contributed to the successful outcome obtained in this case. Most importantly, the patient was very compliant with the bracing and rehabilitation program, and because of his above average base-fitness level was able to perform advanced postural rehabilitation exercises.
Conclusion
This case demonstrates that a severe curve could be reduced to a moderate curve which no longer requires surgery using bracing and scoliosis specific rehabilitation. This case provides evidence that the right treatment, when applied in a consistent manner, can be used to affect change in cosmetic appearance and curve magnitude.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patients type and severity of scoliosis.
© ScoliCare
